What is Goldenhar Sydrome?
Goldenhar Syndrome, sometimes called Hemifacial Microsomia (HFM) or oculo-auriculo-vertebral (OAV) dysplasia, was first recognized by Maurice Goldenhar in 1952. It is an extremely rare condition, affecting approximately 1 out of every 3,000-5,000 births (Barbosa, Cavalcanti, Baptista, Correia, & Carlos, 2003). According to the National Cranio-Facial Association Goldenhar Syndrome is, “a congenital birth defect which involves deformities of the face" ("Goldenhar syndrome," 2009). In 1963, anomalies of the vertebrae were added to symptoms of Goldenhar Syndrome (Healey, Letts, & Jarvis, 2002). In addition to the issues related to the head and spinal column patients with Goldenhar Syndrome may also have problems with their heart and kidneys. One unique characteristic of Goldenhar Syndrome is that it typically affects only one side of the body (Ishmael, 2002).

Symptoms
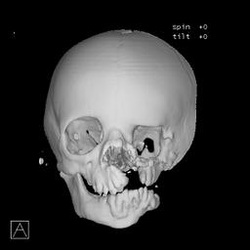
Symptoms of patients with Goldenhar Sydrome vary greatly in severity (Ishmael, 2002). Most frequently Goldenhar Syndrome only structurally affects the face, it typically includes: "a partially formed or totally absent ear (microtia), the chin may be closer to the affected ear, one corner of the mouth may be higher than the other, benign growths of the eye, or a missing eye" ("Goldenhar syndrome," 2009). Patients with Goldenhar Syndrome may also exhibit "..ear abnormalitites, periauricular tags, anotia, mandibular hypoplasia, orbital dystopia, cervical spine anomalies and ocular dermoids. Cranial nerve palsies as well as multiple central nervous system anomalies can also be present" (Clawson, Palinski, & Elliott, 2004). In up to 70% of individuals with Goldenhar Syndrome, "these anomalies are asymmetric and unilateral. During speech and swallowing, the movement of the affected side of the oropharynx and larynx is decreased in comparison to the unaffected side. In children with bilateral presentations, movement of both sides is decreased or absent" (Clawson, Palinski, & Elliott, 2004).
Several developmental issues can occur in children with Goldenhar Syndrome ranging from physical movement issues to problems with cognitive development. Sava states, "There can also be problems with the child's spinal column, and vertebrae may be missing, not properly developed, or they can even be fused together. It is very common for people with Goldenhar Syndrome to have scoliosis. In some cases, children may have mental retardation or a delay in development. Your child may have hearing problems, weakness in one side of face, dental and tongue issues, etc. The symptoms will vary based on the severity of this condition. Goldenhar Syndrome has been seen in all ethnicities, but has been seen to affect males more often" (Sava, 2009). In addition to the problems listed above, a child with Goldenhar syndrome may have weakness on one side of the face, dental problems, and fusion of the bones of the neck ("Goldenhar syndrome," 2009).
Due to the nature of the syndrome and the parts of the body it affects, daily tasks can sometimes be difficult for children with Goldenhar Syndrome. E.P. Clawson et. al in their article regarding feeding difficulties stated, "The facial anomalies associated with Goldenhar Syndrome and the surgery these children often go through lead to multiple feeding problems in children with this disorder. Feeding difficulties related to facial anomalies can include an under-developed maxilla or mandible, hemifacial microsomia, high arched palate, facial palsy, malocclusion, cleft lip and/or cleft palate, crammed teeth and irregularly developed pharynx, palate or tongue" (Clawson, Palinski, & Elliott, 2004). Because of the underdevelopment that frequently occurs in the Mandible and Maxillla the teeth do not occlude correctly, this leads to an innability to properly chew and therefore swallow food. Without proper nutrition patients with Goldenhar Syndrome will become weaker and babies will fail to thrive. Nutrition is vitally important for an individual with Goldenhar Syndrome.
Several developmental issues can occur in children with Goldenhar Syndrome ranging from physical movement issues to problems with cognitive development. Sava states, "There can also be problems with the child's spinal column, and vertebrae may be missing, not properly developed, or they can even be fused together. It is very common for people with Goldenhar Syndrome to have scoliosis. In some cases, children may have mental retardation or a delay in development. Your child may have hearing problems, weakness in one side of face, dental and tongue issues, etc. The symptoms will vary based on the severity of this condition. Goldenhar Syndrome has been seen in all ethnicities, but has been seen to affect males more often" (Sava, 2009). In addition to the problems listed above, a child with Goldenhar syndrome may have weakness on one side of the face, dental problems, and fusion of the bones of the neck ("Goldenhar syndrome," 2009).
Due to the nature of the syndrome and the parts of the body it affects, daily tasks can sometimes be difficult for children with Goldenhar Syndrome. E.P. Clawson et. al in their article regarding feeding difficulties stated, "The facial anomalies associated with Goldenhar Syndrome and the surgery these children often go through lead to multiple feeding problems in children with this disorder. Feeding difficulties related to facial anomalies can include an under-developed maxilla or mandible, hemifacial microsomia, high arched palate, facial palsy, malocclusion, cleft lip and/or cleft palate, crammed teeth and irregularly developed pharynx, palate or tongue" (Clawson, Palinski, & Elliott, 2004). Because of the underdevelopment that frequently occurs in the Mandible and Maxillla the teeth do not occlude correctly, this leads to an innability to properly chew and therefore swallow food. Without proper nutrition patients with Goldenhar Syndrome will become weaker and babies will fail to thrive. Nutrition is vitally important for an individual with Goldenhar Syndrome.